Craniofacial Development and Growth
Since I see individuals from all ages, and a lot of children, it’s important to know the stages of growth in the craniofascial system, and how this applies to the patterns you have now. As you age, there are a lot of things that can drastically change within the cranial system. This and the way we bite (occlusion) can have an affect on our entire bodies.
Let me first give a little anatomy on some of the cranial bones.
Where you have occlusion (bite) changes is through two main bones. The mandible and the maxilla. The maxilla is where your upper teeth erupt from, and the mandible where your lower teeth.

Your maxilla is connected to all the other bones in your head. And the mandible is only connected to your head through ligaments and muscles attaching it to the temporal bone (TMJ).
Okay, now back to the topic…..
The brain and the eyes of infants are more developed than the rest of their bodies. If you notice, newborns have large eyes and noggins and have a small facial structure.

Their nasal cavity is at the same level as the orbital rim, the bone called the mandible is underdeveloped, and the face will appear broad and flat.
Then, an acceleration of vertical growth of the face occurs in relationship to the cranium and continues to grow downward. The sinuses are dependent on this vertical maxillary growth. Teeth start to come out and the mandible starts to grown down and forward to maintain occlusion (bite) with the upper teeth.
At the age of 10, the bones of the head and orbits are almost fully developed, but the maxilla and mandible continue to grow.
Around puberty, the facial structure experience a surge of growth. By adulthood the cranium has grown 60% over its birth size, while the face has grown 93%.
The maxilla, usually is done growing around the age of 12, while the mandible continues to grow until the age of 20. This is a really important part!!!!!
What are some factors that control the growth of these bones????
Genetics– There are some genetic qualities that can affect the proper growth of these bones. Mainly the skull tissue, adjacent structures, growth at brain and eyes, and hormonal influences.
Non-genetics- Non genetic factors that can control the growth of these bones include: the external environment, food, oxygen, chewing and trauma (birth).
Stages of tooth growth
1. Birth to complete primary teeth
2. The first inter transitional period
3. The first transitional period
4. The second inter-transitional period
5. The second transitional period
6. Adult teeth.
*During these inter-transitional periods, you can’t see the external appearance of the teeth, or they remain the same, but the tooth crowds and the roots are developing even though you can’t see them.
- At 7-8 months of age all the teeth except the second and third molars are present and developing
- At 1 year normal and desirable development will start spacing between the teeth
- At 14 months of age the first primary molars appear.
- At 2 1/2 years of age the canines and second primary molars have erupted
- At age 6-8 permanent first molars erupt posterior to the primary teeth. The 8 incisors are replaced by new teeth.
- When there are primary AND permanent teeth this is called Mixed dentition.
Now, I am NOT a dentist, but it is important to know these age ranges and particularly important to know the ages of the maxilla and mandible growth. There can be instances when these bones are not growing properly because of genetics or external factors, and it’s important to screen kids before the age of 12 when that maxilla is done growing, to avoid problems in the future. The typical age I screen children is 8-10 years old.
If these bones are not growing properly, the teeth of course will grow in a way that is abnormal as well. This is what can cause problems with the bite. If there is an abnormal bite, than the forces will go into your head unevenly and can cause a myriad of symptoms.
There are 3 classes of malocclusion ( basically your bite is not normal)
Class I- This is the normal. The balance between the mandible and the maxilla is perfect
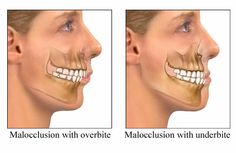
Class II- the mandible is behind the maxilla
Class III- the mandible is anterior the maxilla

For class I, the normal bite, you want three things to occur. 1. proper functioning at the TMJ on both sides. 2. Proper mandibular movement 3. Proper contact at the posterior teeth bilaterally.
You really want most of the contact to be at the back of the teeth, or else when you bite or clench and the forces are in the front, they will go right into your head. This is where headaches, TMJ chronic pains stem from.
If you have a Class II or III occlusion, this can be very traumatic to the head and cranial bones as well as your entire body. This can lead to things as most of you have heard such as overbite, crossbites, ect.
There is a reason your teeth are the way that they are! When I do screening on kids and they are having issues, it is most commonly that the maxilla is too narrow. This causes the teeth to crowd, and tons of symptoms later on down the line. That’s why it’s important to screen early so we can grow them out of these issues.
Also, important is FUNCTIONAL orthodontia. Just making the teeth straight, does not solve any issues, and most people come out of braces with more migraines and headaches than before. That is because you haven’t changed the pattern. The teeth come out of the bones of the head, so if you don’t balance the system, and move the teeth in a way of perfect occlusion, nothing will change. Case in point I had orthodontia, that made my teeth straight, but my bite is totally messed up, which caused me to clench my teeth and have chronic migraines. The way your teeth hit is super important to your function!
The same goes for “invisalign” and using those clear upper teeth retainers. Invisalign cannot fix occlusion (bite) patterns, it can only tip your teeth to move them into being straight. Since the maxilla is connected to all the other bones, invisalign and clear retainers lock these bones in place and don’t allow them to move through their normal patterns of respiration. This can cause more dysfunction and pain. And most the time who perscribes invisalign? Dentists. This is because they don’t have to go to extra school to be able to use them for patients, and can get paid the same amount as braces. Win, win for them. Trust me, there’s a reason orthodontists have extra schooling! You want someone who is knowledgeable about occlusion. I can’t tell you how many people i’ve seen that have had invisalign, or wear the clear retainers, and have chronic headaches. You don’t want any upper nightguards or retainers locking these bones in place. If someone is a heavy clencher, I work with functional dentists to do a lower splint custom made for these patients.
It can get way more advanced, but these are the basics to the growth of your cranio fascial bones. As you see, you have to look at multiple systems, and I’ve had to get knowledge of functional dentistry and orthodontia. Screening kids is super important, as well as having great referral partners when they need them.
If you or anyone you know is suffering from any of these conditions, please don’t hesitate to tell them about my services.!
That is all for now.
Wishing you all a happy and healthy week.
Dr. Hamel